
Dental assistants are often the ones who keep dental unit waterline compliance on track. You already juggle patient care, sterilization, equipment maintenance, chair turnover, and scheduling, so when it comes to waterline safety, the process needs to be straightforward, predictable, and clinically sound.
One of the most important — and sometimes overlooked — principles in routine dental unit waterline management is this:
Dental unit waterlines should be tested before they are shocked, not after.
Testing before shocking gives you insight into what is really happening inside your waterlines, and whether your current treatment products and existing maintenance protocol are actually effective.
Why Testing Your Waterlines is Important
Here’s the deal: the problem is not your water; it’s your waterlines. Your water could be perfectly clean upon entering the operatory, but if there is bacterial buildup in your waterlines, your water becomes contaminated very quickly.
There are multiple examples in the news of these bacteria making patients sick; and when they’re aerosolized, dental staff are also at risk. To minimize this risk, it’s important to monitor your water and keep the bacterial level below the CDC’s recommendation of 500 CFU/mL of water.
The part that many dental teams miss is that the order of your treatment matters.

Why Testing After Shocking Doesn’t Work
Shocking dental unit waterlines is a corrective procedure. It is designed to reduce bacteria and biofilm when levels have exceeded the CDC’s recommended limit of 500 CFU/mL of heterotrophic bacteria.
When you test after shocking, you are only answering one question:
“Did that shock treatment work?”
But that leaves several critical questions unanswered:
- What were your CFU levels before shocking?
- How long has your water been above recommended limits?
- Is your daily maintenance effective, or is it declining over time?
- Are certain operatories performing worse than others?
- Are there systemic issues contributing to biofilm growth?
- Do you have a biofilm problem?
Without a pre-shock baseline, you lose valuable diagnostic information. Bacteria counts may drop after a shock treatment, but if biofilm has already established a home in your waterlines, that treatment will be temporary and the levels will rise again. Testing helps you ensure that your biofilm problem (if you have one) is being addressed.
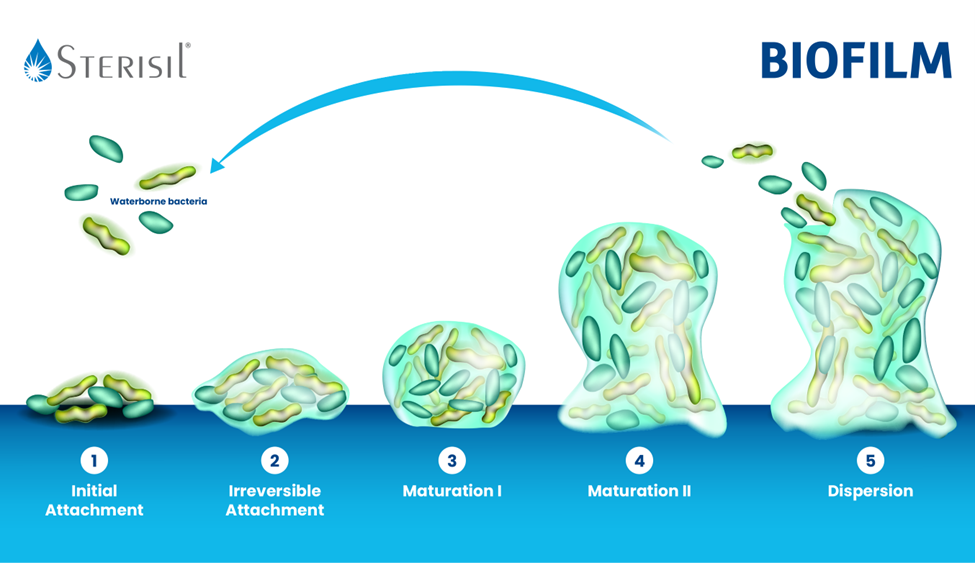
Biofilm Formation Is Constant (And Fast)
Bacteria can duplicate every 4-20 minutes in untreated water. And dental unit waterlines provide an optimal environment for its growth. These are some of the most common factors that speed up biofilm growth:
- Water stagnation in small-diameter lines (like if you don’t treat your waterlines before a holiday closure, for example)
- Infrequent maintenance
- Inadequate shocking protocols
- Dead legs or seldom-used lines
- Low-flow usage patterns
- Breakdowns in process consistency
- High mineral content feeding bacterial growth
If your office only tests after shocking, you may unknowingly operate for extended periods with elevated CFU levels, which puts patients and staff at risk of infection.
Testing before shocking gives visibility into biofilm progression — not just remediation.
It allows you to answer clinically relevant questions, such as:
- Are our levels trending upward?
- Do we need to adjust maintenance schedules?
- Are training gaps contributing to inconsistent results?
- Is our current system sufficient, or just barely holding?
This turns waterline care from reactionary management into proactive quality control, saving time, money, and stress.
Pre-Shock Testing Strengthens Compliance Documentation
Regulators and inspectors value data integrity. A robust dental unit waterline compliance record should demonstrate these things:
- Baseline condition — your test results.
- Corrective action (if applicable) — proof that a shock treatment or other method of remediation was performed.
- Outcome of remediation (if applicable) — post-shock test results confirming success.
This creates a defensible audit trail.
Testing only after shocking removes the baseline component, which weakens documentation and leaves uncertainty in your compliance history.
For practices committed to risk reduction and regulatory confidence, pre-shock testing is a best practice.

The Logic Behind the Sterisil SAFEWaterSolution
Sterisil’s SAFEWater Solution methodology features testing as the first step; it was developed to support predictable water quality management using a structured, clinically rational approach:
1. Test
Gain visibility into current microbial levels before performing corrective treatment. This establishes a benchmark and helps guide decisions.
2. Shock
According to a study of the different approaches you can take when treating and monitoring dental unit waterlines, the most reliable long-term protocol that yields the highest pass rate is pairing routine shock with daily antimicrobial treatment (for example, shocking consistently and using a Sterisil® Straw).
This way, you’re more likely to pass your tests, and if you don’t pass, then remediation will not be as devastating.
3. Maintain
Daily treatment, such as straws or daily tablets, maintains control, rather than repeatedly correcting the system after biofilm has already established.
What Sets the Sterisil SAFEWater Solution Apart from Other DUWL Protocols
The Sterisil SAFEWater Solution features products that were designed to work better together. Because you have a system with compatible products, your protocol is easier to understand, it’s more affordable, and it takes less hours out of your day.
Every step in the protocol is powered by silver ion technology, a high-efficacy treatment method designed to work with any level of water quality. This minimizes user-error and is guaranteed to keep your CFU levels at 10 CFU/mL (50 times less than the CDC’s recommended level).

Why This Matters in Daily Practice
For dental assistants, a “test-before-shock” protocol results in:
- Better visibility into real-world performance
- Clearer documentation during inspections
- Reduced uncertainty about patient risk
- More predictable outcomes after shocking
- Improved confidence in maintenance systems
Most importantly, it reinforces what matters most: delivering safe care without ambiguity.
Testing dental unit waterlines before shocking is essential for establishing baseline conditions, strengthening compliance documentation, and maintaining predictable water quality.
It’s a simple process improvement with meaningful clinical impact.
If your practice wants to improve standardization, confidence, and clarity around waterline management, the Sterisil SAFEWater Solution provides an evidence-based framework that supports testing, treatment, shocking, and monitoring, all working together.
Learn more about how the Sterisil SAFEWater Solution helps practices maintain high-quality dental unit water safely, consistently, and with less uncertainty.



